




October 14, 2016
We continue with the next and final installment in the series republished with permission of the author from the Vaccine Papers website on the scientific proof that vaccines cause autism. In previous installments it was demonstrated that autism is characterized by high levels of brain inflammation including the cytokine interleukin-6 (IL-6), that immune activation resulting in high levels of IL-6 in the developing brain is a necessary and sufficient condition to cause autism in mice and monkeys, and that postnatal immune activation can cause similar conditions to prenatal immune activation. Part 5 is the last piece of the puzzle, specifically linking immune activation caused by vaccines to high levels of IL-6 in cerebrospinal fluid (CSF) by presenting the evidence that vaccines cause febrile seizures, which in turn causes spikes in IL-6 concentration in CSF. In addition, the aluminum adjuvants contained in many vaccines can settle in the brain causing chronically high levels of IL-6. There is evidence that both acute spikes and chronic long-term elevated IL-6 can cause the brain changes we call autism.
There is a great deal more on aluminum on the Vaccine Papers website, and we may be hosting some of those papers as well in the future.
Early-life immune activation has been well-established to regulate the programming of brain development and influence behavior in later life . . .
-Dr Zhibin Yao et al., 2016, Sun Yat-Sen University (Consistently ranked among the top 10 universities in mainland China)And what does a vaccination do? It activates the immune system. That’s the point of vaccination. (emphasis in original)
-Dr Paul Patterson of CalTech: Leading Autism and Immune Activation Researcher, 2006
The cytokine interleukin-6 (IL-6) is produced by the immune system or brain in response to some types of inflammation. Prior articles on immune activation established that elevated IL-6 in the brain causes autism. The scientific evidence proving IL-6 causes autism is described here: “Part 2: Interleukin-6 and Autism.”
Obviously, vaccines cause immune activation. But mere immune activation isn’t enough to argue that vaccines cause autism or brain damage.
In order to establish that vaccines can cause autism and other brain damage via immune activation, we must show that vaccines can stimulate IL-6 in the central nervous system (CNS), in amounts high enough to cause brain damage. This is a challenge, for several reasons:
1) A normal vaccine reaction causes a mild cytokine increase, or no cytokine increase. This is not surprising, because most of the time vaccines do not cause autism, fever or brain damage. Consequently, we are only interested in unusual outliers: adverse vaccine reactions.
2) Cytokine levels in the brain/CNS of living humans can only be measured by obtaining a sample of cerebrospinal fluid (CSF). This creates a difficulty because obtaining a sample of CSF from humans requires a spinal tap, an invasive and delicate procedure. CSF can only be obtained from humans when medically indicated. Therefore, there are no controlled studies that measure cytokines in CSF after vaccination in humans, and never will be.
3) For any individual case, it is difficult or impossible to prove that vaccination is the cause of an adverse event.
These facts make it difficult, but not impossible, to establish a link between vaccines and elevated IL-6 in the CNS.
The link is established by showing that vaccines cause febrile seizures, and showing that febrile seizures always cause high IL-6 in the brain. This line of reasoning is the subject of the present article.
Also, evidence is presented that aluminum stimulates IL-6 in the brain.
Vaccines and Seizures
It is well proven and universally accepted that vaccines can cause febrile seizures (a seizure in combination with fever). The only disputed issues are the incidence of seizures resulting from vaccines, and whether they can cause long-lasting damage. The phenomenon is difficult to study because of healthy user bias (i.e. because children with pre-existing health problems receive fewer vaccines, explained here: “Healthy User Bias”), and because vaccine-induced seizures can occur several days or (at least) about 2 weeks after vaccination.
Nevertheless, it is generally accepted that vaccines are the second-leading cause of febrile seizures in children. Citation: “Vaccines and Febrile Seizures”
One of the best studies on vaccines and seizures is a 2011 Canadian “self-controlled” study by Wilson et al. Self-controlled studies use the same subjects for both control and exposed groups. Subjects are compared to themselves at different points in time. In Wilson et al., health outcomes in a “risk period” (4-12 days after vaccination) are compared with a later “control period” (20-28 days after vaccination). This study design avoids the problem of healthy user bias. Paper (Wilson et al.): “Adverse Events Following 12 and 18 Month Vaccinations”
The Wilson study is based on the assumption that vaccines are unlikely to cause seizures more than about 20 days after vaccination. This assumption is of course debatable, and to the extent it is wrong, the study will tend to underestimate the seizure risk of vaccination. In other words, the risk will be underestimated if vaccines cause adverse events in the control period of 20-28 days.
Self-controlled studies of vaccine adverse effects can only be used for acute, rapid-onset reactions. It is not possible to use the self-controlled study design to investigate adverse effects with delayed onset (e.g. autism).
Wilson et al. looked only at the 12- and 18-month vaccination dates. At the 12-month date, children in Canada receive the MMR, meningococcal, pneumococcal and varicella vaccines. Vaccines given at 18 months are fewer and more variable, according to the schedule: Canadian vaccine schedule.
Wilson et al. found an increased risk of febrile seizures (20 per 100,000) and emergency room (ER) visits (598 per 100,000) associated with the 12-month vaccination date in the risk period, compared to the control period. The study observed a smaller increased risk at the 18-month date. Some of the 598/100,000 adverse events requiring ER visits likely include brain inflammation.
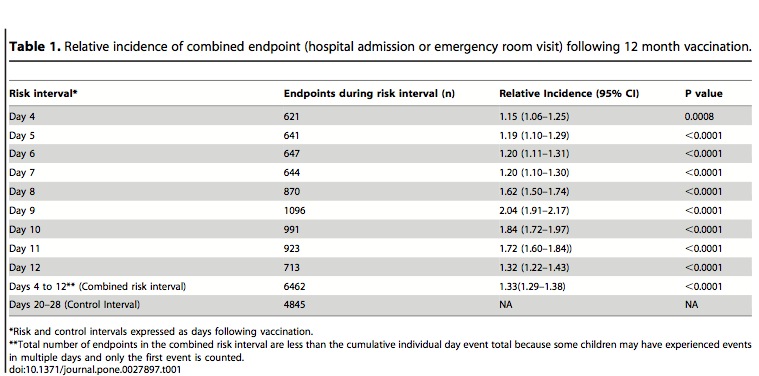
Above: Emergency room visits are elevated on days 4-12 after 12-month vaccination date (in Canada), compared to days 20-28 after vaccination. From Wilson et al. 2011
The number of vaccines at the 12-month date is comparable to the 2-, 4- and 6-month dates, which in sum call for 3 doses of DTaP, HiB, rotavirus, and Hep B vaccines, and one dose (at one of the 2-, 4-, or 6-month dates) of pneumococcal and meningococcal vaccines.
Another study by MacDonald et al. of the MMR, varicella and MMRV (MMR + varicella) vaccines found a risk of febrile seizures of 35 per 100,000 for the MMR + varicella vaccine given separately, and a risk of 70 per 100,000 for the combination of MMR+varicella (the “MMRV vaccines). The addition of varicella to the MMR vaccine doubled the risk of febrile seizures. In view of this result, the risk of febrile seizures from combining vaccines may be synergistic (i.e. greater than merely additive). Paper (MacDonald et al.): “Risk of Febrile Seizures After First Dose of Measles-Mumps-Rubella-Varicella Vaccine: A Population-Based Cohort Study”
Not all vaccines have been studied as a cause of febrile seizures, but the influenza vaccine and DTaP vaccines are also known to cause febrile seizures, though at a lower rate than MMR. it is doubtful however that the true rate of seizures from DTaP are known.
At the 2-, 4-, and 6-month dates, 8, 7, and 9 vaccines (respectively) may be given simultaneously according to the U.S. CDC vaccine schedule.
If the risk at the 2-, 4-, and 6-month dates are comparable to the 12-month date in the Wilson study or MacDonald study, the total fraction of children suffering febrile seizures will exceed 1/1000.
Also note that it is difficult to diagnose a seizure in a young infant. They are easily missed. In a hospital setting, observing a seizure in an infant typically requires electroencephalograph (EEG) monitoring. So the true rate of vaccine-induced seizures in infants is unknown. The true rate of seizures and brain inflammation from 0-, 2-, 4-, and 6-month vaccines may be substantially higher than the rate for MMR or the 12-month vaccines.
Seizures and Cytokines
A small increase of IL-6 in response to trauma or infection protects the brain. Too much IL-6 is damaging and causes autism.
A number of studies have been performed on the cytokine response to seizures. These studies are consistent: Febrile seizures are strongly associated with increased IL-6 in the CSF and blood. The evidence indicates that seizures stimulate IL-6 production in the CNS.
Normal levels of IL-6 in human CSF are about 1-5 pg/mL, and more typically about 1-3 pg/mL.
There is only one study reporting CSF levels of IL-6 in children and infants with febrile seizures: Ichiyama 2008.
Other seizure studies cited here report IL-6 levels in blood and/or CSF and in response to various kinds of seizures (febrile and non-febrile) in adults and from causes different from acute vaccine adverse reactions (e.g., alcohol withdrawal, epilepsy). However, these other studies are still relevant because seizure per se causes the production of IL-6 in the CNS.
Ichiyama 2008
This paper reports IL-6 and other cytokine levels in blood serum and CSF after febrile seizures, with (n=13) and without (n=23) “acute encephalopathy.” Subjects in this study were children, with many younger than 18 months. Encephalopathy is generally defined as alteration of consciousness in combination with slow activity on EEG (which is abnormal and indicative of brain dysfunction). In cases of febrile seizure without encephalopathy, CSF IL-6 could be as high as 400-500 pg/mL (estimated from Fig. 2, below). This is about a 100-400 fold increase in the CSF over typical baseline (1-3 pg/mL). IL-6 levels may be even higher if encephalopathy is present. Paper (Ichiyama et al.): “Serum and CSF Levels of Cytokines in Acute Encephalopathy Following Prolonged Febrile Seizures”
Ichiyama also found that in cases of encephalopathy, IL-6 is almost always higher in CSF than serum. This is expected if the brain is producing IL-6, as is commonly believed (by researchers in this field) to be the case.
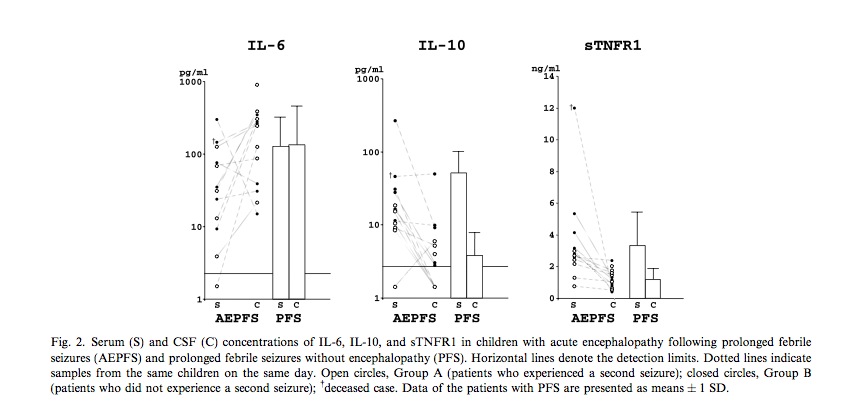
Above: Febrile seizure can produce about a 100-400-fold increase of IL-6 in the CSF, compared to normal baseline (1-3 pg/mL). Notice that unlike other cytokines IL-6 is typically higher in cerebrospinal fluid (CSF) than blood serum, indicating that the IL-6 is produced inside the central nervous system (CNS). From Ichiyama et al. 2008.
PFS=Prolonged febrile seizure
AEPFS: Acute encephalopathy + PFS
S=Serum measurements
C=CSF measurements
IL-6 levels in CSF spike within a few hours after seizure, and return to baseline in about 24-48 hours. IL-6 levels in CSF change rapidly, and consequently it is not possible to determine the peak IL-6 level. In the Ichiyama study, there is only one measurement per subject, and this measurement could be before or after the peak in IL-6. So, a “low” IL-6 measurement does not necessarily mean that the subject did not experience a high peak IL-6. It is very likely that all seizures produce a spike in IL-6.
Brain IL-6 in Immune Activation Experiments
The CSF IL-6 level in febrile seizures can be compared to the IL-6 level in the immune activation experiment of Oskvig et al. (cited in the postnatal immune activation article: “Part 4: Postnatal Immune Activation”). In the Oskvig experiment, a pregnant mouse was injected with lipopolysaccharide (LPS) to stimulate immune activation, and IL-6 was measured in the fetal brain 4 hours and 24 hours later. Oskvig reported IL-6 concentrations as pg/mg protein* (which is different from pg/mL used for CSF). Controls had about 4 pg/mg IL-6 (estimating from chart at right), and immune activation-exposed fetal brains had about 675 pg/mg at 4 hours, and 240 pg/mg at 24 hours. Hence, the immune activation caused 169-fold (@4h) and 60-fold (@24h) increases in IL-6 compared to controls. These mice displayed autistic behavior.
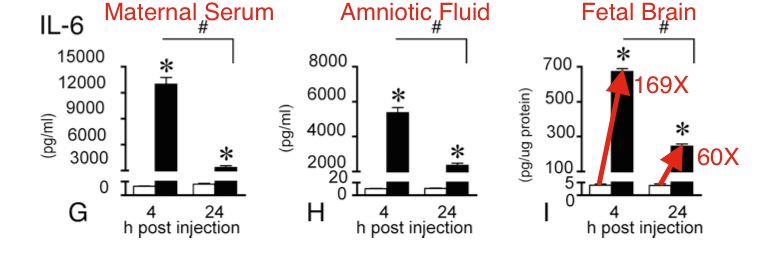
Above: IL-6 measurements in maternal serum, amniotic fluid, and fetal brain 4 and 24 hours after immune activation. The increase in fetal brain IL-6 (169- and 60- fold at 4 hours and 24 hours, respectively) is comparable to the increase in IL-6 observed in human CSF after febrile seizure. The mice in this experiment displayed autistic behavior. From Oskvig et al. 2013.
The single, short-duration spike in IL-6 observed in Oskvig et al. is sufficient to cause brain damage and autistic behavior in the mice. Hence, it is reasonable to expect that the comparable increases of IL-6 observed after febrile seizures in infants will cause similar brain damage and autism in humans.
It is possible that the immune activation also causes a milder chronic IL-6 elevation in the brain, and that the chronic exposure is what causes the damage. The Coiro experiment, for example, observed that an anti-inflammatory drug (ibudilast) given postnatally prevented the damage and autistic behavior. Also, the Wei et al. experiment observed autistic behavior and physical changes from chronic IL-6 exposure. Precisely when the damage occurs is unknown at this time, but there is evidence that both acute and chronic IL-6 elevation can cause the damage. Paper (Coiro et al.): “Impaired Synaptic Development in a Maternal Immune Activation Mouse Model of Neurodevelopmental Disorders”
One Flawed Study of IL-6 in Seizures
An earlier study by Ichiyama in 1998 failed to observe an increase in IL-6 in CSF following febrile seizures in 20 subjects. However, this study has been criticized for delayed collection of CSF samples. IL-6 in the CSF is transient and disappears in about 24-36 hours after seizure. Ichiyama collected CSF samples for analysis about 26 hours after the seizure, on average. Peltola (2000) states the following about the Ichiyama study:
. . . time is an important factor to consider when determining the CSF levels for IL-6. In our previous study elevated CSF levels of IL-6 were detected in 27% of patients with seizures occurring within 72h before sampling, on the other hand all increased IL-6 levels were observed in patients sampled within 15 h from the seizure.
and
In that study (Ichiyama 1998), CSF samples were taken on days 1-2 (mean 1.1 +/- 0.2), but in our previous study none of the samples studied later than 24 h from the seizure were positive.
[Emphases added unless otherwise stated.]
Another paper (also by Peltola et al.) states “Our results suggest that seizure-related IL-6 production occurs rapidly and is transitory . . . .”
In order to detect the IL-6 spike, the CSF sample must be obtained soon after the seizure. This explains why Ichiyama in 1998 failed to observe elevated IL-6 in CSF.
This paper (Ichiyama 1998) is mentioned because some vaccine advocates have used it to argue that seizures do not stimulate IL-6 in the brain. This argument is wrong.
All Seizures Stimulate IL-6 Production in CNS
Researchers in this field believe that seizure brain activity per se stimulates IL-6 production in the brain. This opinion is based on human observations and animal experiments. IL-6 is known to be rapidly produced following different kinds trauma and inflammation. For example, physical trauma to nerve tissue is known to induce IL-6 production within hours, well before other cytokines.
Peltola, 2000
In this study, IL-6 was measured in CSF and plasma shortly after seizures, with the goal of understanding the time course of IL-6 production and relationship with other cytokines.
Peltola states
The mean concentrations of IL-6 were significantly increased in CSF (P<0.001) and plasma (P<0.01) after tonic–clonic seizures.
and
We provide evidence of intrathecal production of IL-6 associated with electrical seizure activity. [Intrathecal = Inside the CNS. Refers to the spinal theca, which is filled with CSF.]
and
We have previously reported increased concentrations of interleukin-6 (IL-6) in CSF from patients with newly developed tonic–clonic seizures without any evidence of infection or CNS trauma, where increased cytokine production most likely is a consequence of neuronal epileptic activity associated with seizures (Peltola et al., 1998).
and
The cytokines measured in CSF can be either of peripheral blood or intrathecal origin . . . . The mean concentrations of IL-6 in our study were higher in CSF than in plasma (22.0 pg/ml vs. 3.8 pg/ml) supporting the hypothesis of intrathecal production of IL-6.
Paper (Peltola 2000): “Interleukin-6 and Interleukin-1 Receptor Antagonist in Cerebrospinal Fluid from Patients with Recent Tonic–Clonic Seizures”
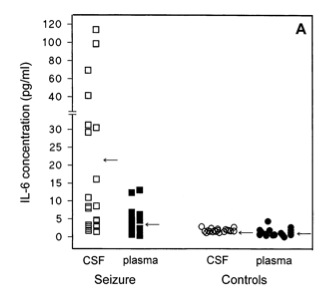
Above: CSF and blood plasma levels of IL-6 after seizures in adults (age 15-60), and in healthy controls. Note that after seizure, levels are often higher in CSF than plasma, implying that IL-6 is produced in the CNS. From Peltola et al 2000.
Lehtimaki, 2004
This study is essentially a replication of the earlier Peltola study, by the same research group, and it explored the effect of seizure type. Repeated and single tonic-clonic (i.e. “grand mal”) seizures and partial seizures were compared in their effects on IL-6 production. This study found further confirming evidence that seizures stimulate IL-6 production in the brain. Lehtimaki states
In patients with recent GTCS, we have previously found a rather selective increase in the levels of IL-6… (Peltola et al., 1998, 2000a). The present study confirms and further extends these findings. The levels of IL-6 both in CSF and in serum were increased in all seizure groups…the magnitude of the IL-6 activation was most pronounced in patients with recurrent GTCS, i.e. in the case of most severe cerebral epileptic activity. These human data seem to be consistent with experimental studies suggesting that the secretion of IL-6 may be induced by seizure activity per se (Jankowsky et al., 2000, Sallmann et al., 2000).
and
These results provide further support for a hypothesis of cytokine production induced by seizure activity per se.
GTCS=generalized tonic-clonic seizure, formerly known as “grand mal.” A tonic-clonic seizure affects the entire brain.
PPS=prolonged partial seizure
Paper (Lehtimaki 2004): “Regulation of IL-6 System in Cerebrospinal Fluid and Serum Compartments by Seizures: The Effect of Teizure type and Duration”
In view of this evidence, any seizure, including those caused by vaccines, stimulates IL-6 production in the brain. Since vaccines cause febrile seizures, and IL-6 causes autism, the implications are obvious.
Autism and Febrile Seizures
If the above analysis is correct, then there must be an association between febrile seizures and autism. If this association is not present, then the above analysis is wrong. A 2012 paper by Zhang et al. reports an association between febrile seizure and regressive autism. Regressive autism comprises about 14-50% of autism cases (depending on how its defined). Regressive autism presents as loss of previously acquired skills, such as loss of language and social skills. Repetitive behavior will appear at the same time. The onset can be abrupt and is often associated with recent vaccination, according to parental reports.
Zhang et al. states
Analyses by multiple logistic regression showed significant correlations between autistic regression and febrile seizures (OR=3.53, 95% CI=1.17-10.65, P=0.025), as well as with a family history of neuropsychiatric disorders (OR=3.62, 95% CI=1.35-9.71, P=0.011).
and
In this study, the prevalence of febrile seizures in autistic regressive individuals is 20.6% (7/34), significantly higher than that in nonregressive autistic individuals (6.6%, 9/136), and both higher than in the general population. In multiple logistic regression analyses, febrile seizures were associated with a significantly increased risk of regression.
Interestingly, the association with autism was about equally strong for febrile seizure and for family history (OR=3.35 for seizures and OR=3.62 for family history). This suggests that both factors may have equally strong tendency to cause autism. Everyone agrees that genetic factors contribute to autism. Febrile seizures may be equally important.
Also, the study found no association between autistic regression and perinatal risk factors (“perinatal”= time period of a few weeks before and after birth). This suggests that the children had normal gestation and birth, and did not suffer injury during birth. This is evidence that the children were normal when born, and were injured by something after birth, like vaccines. This has been a consistent finding in autistic regression. Zhang states
“No significant associations were found between autistic regression and perinatal risk factors, in agreement with the findings of other authors.40,41
Paper (Zhang et al): “Risk Factors for Autistic Regression: Results of an Ambispective Cohort Study”
Below is the main finding of Zhang et al.:
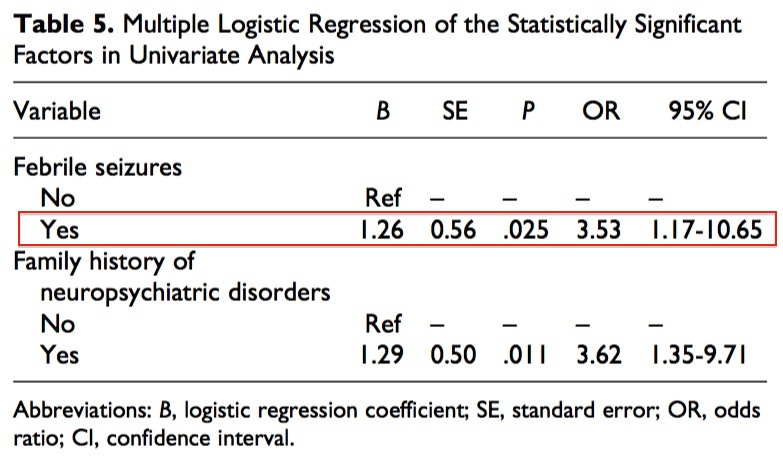
Above: Febrile seizures are associated with regressive autism. The association is strong and statistically significant. The strength of the association is about the same as for family history of psychiatric disorders. This suggests that febrile seizures may have the same power to cause regressive autism as genetics. From Zhang et al. 2012.
IL-6 Exposure Duration
There is evidence that both acute and chronic IL-6 elevation can cause autistic behavior.
Evidence for acute exposure: Autistic behavior can occur (in humans) with rapid onset (described in case reports here: “Part 4: Postnatal Immune Activation”). Also, almost all of the studies of immune activation in animals cause acute exposure of the brain to IL-6 (e.g. Oskvig et al.).
Evidence for chronic exposure: The Wei et al. study (with engineered virus containing IL-6 gene) showed that chronic elevation of IL-6 in the brain causes autistic behavior. Also, the Coiro et al. study in mice demonstrated that anti-inflammatory treatment starting about 7.5 days after immune activation prevents autistic behavior. Both studies indicate that behavioral changes can result from chronic IL-6 exposure.
An acute IL-6 burst (from seizure and/or immune activation) may cause chronic IL-6 overproduction. This type of effect is generally observed in immune activation experiments. Specifically, an immune activation event during early development causes long-term elevated inflammation.
Aluminum Increases IL-6 in the Brain
Immune activation isn’t the only issue. Both ingested aluminum and injected aluminum adjuvant deposit some aluminum in the brain. As of April 2016, there are no scientific papers reporting whether Al adjuvant stimulates IL-6 production in the brain. However, it is known that Al adjuvant stimulates Th2-type immune activation, which is associated with IL-6. The Li et al. paper reported that hepatitis B vaccine caused an increase of IL-6 in rat brain (Fig. 5F). The hepatitis B vaccine contains aluminum adjuvant. Paper (Li et al.): “Neonatal Vaccination with Bacillus Calmette–Guérin and Hepatitis B Vaccines Modulates Hippocampal Synaptic Plasticity in Rats”
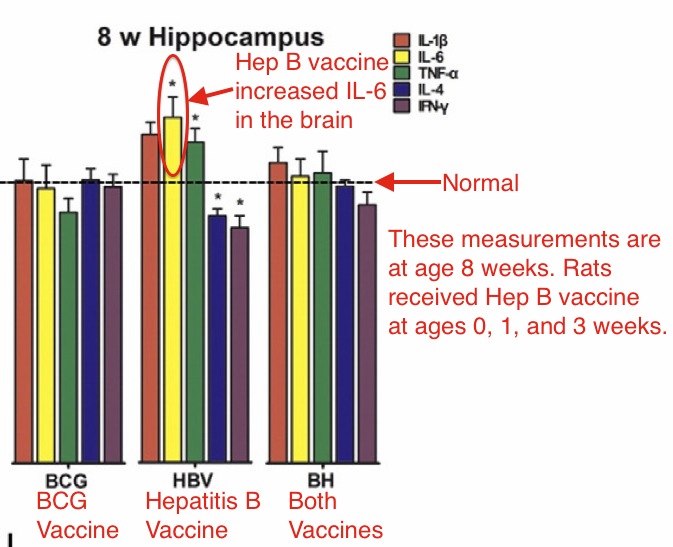
Above: Hepatitis B vaccine caused long term increase in IL-6 in rat brain. TNF-a was also increased; TNF-a is associated with autism. Hepatitis B vaccine contains aluminum adjuvant. From Li et al. 2015.
A recent study (Alawdi et al) measured inflammation in rat brain caused by ingestion of 3.4 mg/kg/day aluminum. Aluminum ingestion increased IL-6 in the brain 4-fold. The aluminum impaired learning and memory and caused numerous behavioral changes. The aluminum also increased many other indicators of inflammation and brain degeneration (e.g. phosphorylated tau protein and amyloid beta, two substances elevated in Alzheimer’s disease). Paper (Alawdi et al.): “Neuroprotective Effect of Nanodiamond in Alzheimer’s Disease Rat Model”
3.4 mg/kg/day is far lower than the 62 mg/kg/day or 26mg/kg/day aluminum dosages claimed to be harmless by Dr Paul Offit and other vaccine promoters. This issue is discussed here: “The Foundation for Al Adjuvant Safety is False.”
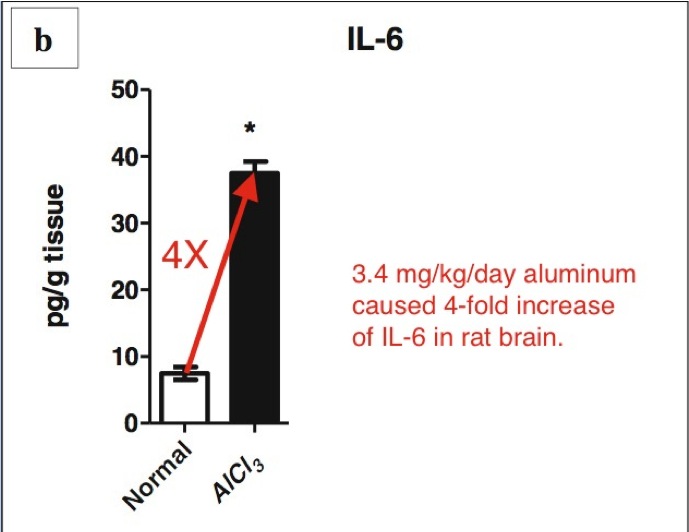
Above: Ingestion of 3.4 mg/kg/day aluminum for 6 weeks caused 4-fold increase of IL-6 in rat brain. Note that 3.4 mg/kg/day aluminum is much lower than the aluminum dosage (62mg/kg/day and 26mg/kg/day) claimed by vaccine advocates (e.g. Dr Paul Offit) to cause no adverse effects in animals. From Alawdi et al. 2016.
The Alawdi et al study used ingested AlCl3, not injected Al adjuvant. There are no published reports of IL-6 levels in brain after aluminum adjuvant injections. Such data is urgently needed and experiments are underway.
Since Al adjuvant can persist in the brain for years, it should be expected that Al adjuvant in the brain may cause chronic, long-term elevation of IL-6. This may be a mechanism for causing autism.
Conclusion
Febrile seizures induced by vaccines stimulate high levels of IL-6 in the brain, in humans. The increase of IL-6 produced by vaccine-induced seizures is comparable to the increase demonstrated to cause autistic behavior in animal experiments.
All these steps have been supported by scientific evidence: vaccination > febrile seizure > IL-6 > autism.
Aluminum is proven to cause chronic inflammation in the brain, including increased IL-6. Aluminum adjuvant can be transported into the brain. Aluminum from vaccines therefore likely causes chronic IL-6 elevation in the brain. Both acute and chronic IL-6 elevation have been demonstrated to cause autistic behavior and brain damage in animals.
The issues of chronic IL-6 elevation, and the inflammatory effects of aluminum will be explored in future articles. Scientific research on aluminum adjuvant and IL-6 (and IL-17a) in the brain is underway (summer 2016).
***************************************
Note: Oskvig et al. contains a typographical error. IL-6 is shown as units of pg/ug (picograms per microgram brain protein), but this is wrong. The correct units are pg/mg, picograms per milligram protein.
For a list of papers in this article, click here.
For a list of the other articles in this series, click here.







************NEWSFLASH ***************
Andrew W is in Italy at the moment , he got invited into the senate to discuss Vaxxed.
The film is all over Italian main stream media.
I am so sorry for your experience. There will be a movie coming out in Spring 2017,…called “The Truth about Vaccines”… watch for it. I have only recently become exposed to this cover-up. There is a very effective movement going on right now on Periscope (app). They are interviewing people all over the USA who have had negative effects from vaccines. It’s harrowing and tragic to listen too.
Posted by: RichardCurtin | October 17, 2016 at 10:01 PM
Note: Oskvig et al. contains a typographical error. IL-6 is shown as units of pg/ug (picograms per microgram brain protein), but this is wrong. The correct units are pg/mg, picograms per milligram protein.
——
We forgive you , great work Vaccine papers\TMR .
——
All these steps have been supported by scientific evidence: vaccination > febrile seizure > IL-6 > autism.
Aluminum is proven to cause chronic inflammation in the brain, including increased IL-6. Aluminum adjuvant can be transported into the brain. Aluminum from vaccines therefore likely causes chronic IL-6 elevation in the brain. Both acute and chronic IL-6 elevation have been demonstrated to cause autistic behavior and brain damage in animals.
Fantastic news indeed :
http://www.irishtimes.com/news/health/ireland-asked-to-attend-who-meeting-over-low-uptake-of-hpv-vaccine-1.2820866
Ireland asked to attend WHO meeting over low uptake of HPV vaccine
Uptake in vaccine to prevent cervical cancer low ‘due to huge impact of lobby groups’
Yes, we’re quite delighted to know that HPV vaccine uptake in Ireland has plummeted.
‘ The scientific evidence proving IL-6 causes autism is described here: “Part 2: Interleukin-6 and Autism.” ‘
Well, you showed altered fear responses in IL-6 treated mice being shocked in a box.
There was a lot more than “altered fear responses in IL-6 treated mice being shocked in a box.” That was just one of a number of behavioral assays that were indicative of autistic behavior in mice, which included social behavior. In addition, the experiment you are referring to analyzed physical brain changes as well.
A 2016 survey of EHS people in Australia found that 100% of resp0ndents were female, over 50 , highly intelligent and sensitive to insect bites. All had amalgam tooth fillings out years ago due to immune system problems. It seems some highly intelligent people have very alert immune systems from birth or even before. People who come under the gifted label have extra neurological connections in the brain. They develop at 140% the usual rate on average until over 70 years. The extra sensitivities are not only physical but emotional and spiritual as well. Women are penetrated by electromagnetic emissions more than men due to extra fluid in their bodes. It is microw3ave radiation after all and their bones are not so dense. Children and unbo9rn babies are most at risk. http://www.australianbiophysics.org and .com are an attempt to make information that seems to be concealed in Australia available for people to learn. In USA and AUS and NZ the radiation levels allowed are 1000 times higher than in EU. The websites are hard to get to . It seems someone does not want you to find them but persevere. Type the address directly into your browser not a search engine.
I still think that our increasing electrical environment with all the escalation of new technologies such as mobile phones, wifi etc. can be causing the problem with vaccinations as I am electrically sensitive now and cannot have vaccinations any more as the blood-brain barrier is damaged and lets metals into the brain whereas when I was a child in the 1940s to 1950s though I was allergic to things I could have all the vaccines without a problem and even into my older age. Also autism prior to new technology was hardly ever a problem despite all of us having vaccinations. Therefore I believe the correct research would be to check the homes of those who become ill after vaccinations and see what electricity exposure these children have as opposed to those who do not react but of course there is too much money in technology for most research to be funded for this. However there is plenty of research proving the damage from technology but people either do not know or do not believe this problem while many suffer around the world and the numbers are escalating.