




April 19, 2017
 There are few things more egregious in the vaccine risk-aware community right now than the HPV vaccine and its tsunami of marketing efforts, targeting one of the biggest fears the American people have: cancer.
There are few things more egregious in the vaccine risk-aware community right now than the HPV vaccine and its tsunami of marketing efforts, targeting one of the biggest fears the American people have: cancer.
HPV is a common sexually transmitted infection, which generally presents no symptoms and clears spontaneously in most people who have it. Only a small percentage go on to ever have problems for which the U.S. has robust screening and treatment programs available. Deaths from cervical cancer are relatively low, which is not to diminish the devastation caused to families affected by this horrific disease.
Despite the over-reaching promises that this vaccine would prevent cancer (Merck has never demonstrated this), with campaigns like “Be One Less,” the vaccine has failed to take a foothold in the mainstream pro-vaccine psyche with “unacceptably low” vaccination levels. There are many reasons, but for me the main one, and the one that Merck, the WHO, CDC and the FDA fails to acknowledge, is the many stories of injuries circulating around the globe. They are trying their best to counter the ever-growing grassroots alarm bells with frightening cancer prevalence statistics at every chance they get, but it’s not working. Vaccine mandates loom in many states, but so far, parents have kept them at bay in 47 of them.
Gardasil marketing campaign
Enter a newer stealth marketing strategy, employing the unequivocal endorsement of various medical professional bodies to push the vaccine on the public from every vantage point. The American Academy of Pediatrics, the American Society of Clinical Oncology, the American College of Obstetrics and Gynecology and even the American Dental Association, to name a few, have all come out with press releases or updated mission statements touting the vaccine as their singular recommendation for good health practice for HPV-related cancer prevention. This recommendation has supplanted educating their patients about avoiding all risk factors, which used to be the norm, and some would say, most risk averse.
I don’t mean to sound like I suspect that there’s some conspiracy here and that Merck is somehow in bed with these reputable organizations in order to sell its drugs and vaccines; I’m saying it’s their business model. Merck pays scientists and doctors all over the world to speak on their behalf, to conduct studies, to analyze market data, and to appear in the media to promote and support the infallibility of their products. Merck also funnels money into medical research, universities, hospitals and even politicians’ coffers. And nowhere has this been more blatant than with Gardasil and Merck’s long-time investment in Women in Government. WIG provides its members with a plug-and-play legislative toolkit to assist in implementing state Gardasil mandates. There’s no man behind the curtain; it’s all out there, hidden in plain sight.
This business model seeks out the collaboration of institutions who have direct influence on those who can actually deliver products directly to customers—practicing doctors—and seamlessly increase the bottom line. After all, the only population Merck has a duty of care to is its shareholders.
The American Academy of Pediatrics is already firmly on board with recommending the HPV vaccine to every one of its patients over the age of nine. But there is another as-yet untapped sales force: the American College of Obstetrics and Gynecology (ACOG).
In 2012, ACOG partnered with “Merck For Mothers” to launch “Saving Mothers,” a noble cause focused on making labor and delivery safer for women in developing nations. (Incidentally, if you have $750 to spare, our old friend from the CDC, Julie Gerberding, is being honored by the NY Academy of Medicine for her work at Merck for Mothers on June 13th, another major medical academy alliance).
In 2010, Merck began supporting vaccination education at ACOG by providing the funding for the website www.immunizationforwomen.org. It serves as the go-to for OB/GYNs where they can find webinars, toolkits, and other resources to assist ACOG members to
“. . . further enhance the role of ob-gyns as vaccinators of adolescent and adult women.”
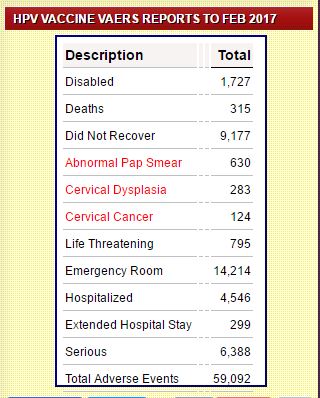
Adverse events of Gardasil from Sanevax.org
During one of these webinars, a really nice doctor (Dr. Jennie Yoost) can be heard advising listeners on how best to convince young adolescents (and their mothers) to get this vaccine at all costs. Indeed, the webinar was devoid of any vaccine risk information or potential side effects other than a sore arm. It did not remind the listeners of the need for regular Pap tests. They were not told how long the vaccine would last (the best guess is five to eight years).
They were encouraged to use scripts and unsubstantiated facts presented out of context to bolster the vaccine’s importance and relevance for U.S. children. Statistics for developing countries were mixed in with developed, skewing the patient’s impression, acting as a subversive form of fear-mongering. All of this is vital information one needs in order to weigh up a reasonable risk-benefit assessment, especially for young children who are not even their patients. It is their mothers who are receiving and processing that information during a “well visit.” Sound familiar?
Then Dr. Yoost was asked the uncomfortable question,
How can we better recommend or encourage boys to get the HPV vaccine, given that the prevalence of anal and penile cancers in heterosexual populations is much lower?
Dr. Y: I’m not sure about the prevalence of those specific types of cancers in heterosexual populations, but as far as messaging, I would stick to some of those messages that we talked earlier about, in talking to young men and women, just their risk of cancer in general . . .
And it’s good to hear Merck-sponsored doctors confirm how world “alphabet organizations” are involved in acting as sales agents for Gardasil by negotiating very low-priced doses, around $10 vs. the $195 U.S. children pay:
And in Rwanda, I think they were able to provide the vaccine for under $10.00 per dose of vaccine . . . Don’t quote me on that . . . (me: Sorry) But the World Health Organization, along with the Gates Foundation, is very—is actively involved in promoting HPV vaccine, because screening is so difficult in these developing countries.
It’s interesting that Rwanda was mentioned because they have a mandatory school-based vaccination program with uptake rates of 95%. My guess is there’s a subliminal message being planted there.
Then you have the ultimate affront to patients, fundamentally destroying what’s left of the doctor-patient relationship (which is built on implicit trust) by encouraging a script with no regard for its truth or lack thereof:
. . . try using these messages . . . Physicians are making sure their own children get the HPV vaccine before they are at risk. Try using an I statement. ‘I made sure my children received the HPV vaccine to protect them against HPV related cancers.’
They even went so far as to absolve doctors of their duty to provide informed consent by telling them (transcripts here)
. . . you can say, “Your child needs these vaccines today,” and name all the vaccines—meningococcal, Tdap, and HPV. Recommend whatever is recommended for the child’s age, so it’s not presented as optional.
In fact, it’s very much an optional medical procedure as it is only mandated in three states and exemptions are available. Doctors are not henchmen for Merck or the state. But as you can see, this is a creeping policy, where something new is added to what initially seems innocuous. And before you know it, there is all-out medical tyranny at play, and no one knows where or how it started.
However, the website tells us that ACOG cannot be influenced by all this generous, agenda-neutral, unbiased information which has been donated by the vaccine’s manufacturer:
This website is supported by an independent educational grant from Merck and an educational grant from Sanofi Pasteur U.S. ACOG does not allow companies to influence its programs, publications, or advocacy positions.
Good to know.
This leads me to ACOG’s most recent committee opinion on the HPV vaccine, released on March 24, three months ahead of schedule. It makes the 2016 opinion sound rather innocuous. The first thing we notice is that 2017’s opinion declares two authors where none was noted in the previous version. Dr. Linda O’Neal Eckert of the University of Washington and Dr. Anna-Barbara Moscicki of UCLA, assisted in preparing the manuscript.
Dr. Linda O’Neal Eckert is a huge proponent of vaccinating pregnant women, has worked with the WHO in Geneva on the HPV vaccine, and has co-authored over 30 papers primarily on immunization and pregnancy. She envisions a new era where OB/GYNs should be at the forefront of vaccinating women, including pregnant women. Her focus seems to be on how to increase coverage and remove barriers to increasing uptake. However, she does have a keen interest in safety, the negative impression of which is a barrier in itself, but she acknowledges the need to improve doctors’ awareness of the VAERS reporting system so that they can become “competent and complete vaccinators.”
Dr. Anna-Barbara Moscicki has received Merck sponsorship and is also an HPV researcher. She has co-authored over 90 studies and is a true expert, so her input into the ACOG new committee opinion is important. Her most recent study looked at how children with HIV developed immunity to four doses of Gardasil. In another study, Dr. Moscicki states that we still don’t understand what actually causes cervical cancer and more research is needed:
Persistent infection with oncogenic human papillomavirus (HPV) is necessary but not sufficient for the development of cervical cancer. The factors promoting persistence as well those triggering carcinogenetic pathways are incompletely understood. Rapidly evolving evidence indicates that the vaginal microbiome (VM) may play a functional role (both protective and harmful) in the acquisition and persistence of HPV, and subsequent development of cervical cancer.
However, neither doctor’s blatant industry ties and conflicts of interest were disclosed on the most recent opinion, just as Dr. Offit was not required to recuse himself from voting in the ACIP meeting on whether to add his own rotavirus vaccine to the schedule even though he would personally benefit financially. Is it okay because everyone’s doing it? Does the fact that it’s just the way things are done somehow negate the conflicts?
The recommendations themselves have taken on a new tone. In the previous opinion, ACOG’s primary mission was to encourage its members to be key educators on the vaccine and to use various tools to persuade them to get it because “safety data is reassuring.”
The tone changes in 2017, where ACOG is now recommending that its members suggest vaccinating at well visits or educating older women about vaccinating their children. OB/GYNs are now told to educate their patients about the entire CDC recommendations for boys and young girls, patient populations they don’t even serve. Genius.

The recommendations then start to mirror the rather insidious nature of the webinar from Merck above. It seems to be saying vaccinate first, ask questions later. It is attempting to eliminate all barriers to vaccinating by making new cohorts of vaccinees not considered before.
Bizarrely, the new recommendation specifically states not to test for HPV DNA before vaccinating, even though it’s a core function of OB/GYNs to test for STIs. It also says that the vaccine is safe even if you have had an abnormal pap test. What? The authors must not have read Merck’s protocol 013 where they found that girls who were sero-positive for vaccine-strain HPV before being vaccinated were 44.6% more likely to progress their infection than those who were sero-negative. I understand this finding has been dismissed because the sero-positive girls may have had other risk factors like smoking, but in the real world young women and girls have a wide variety of risk factors, so doctors should be paying close attention to that clinical trial outcome.
It goes on to support vaccinating while a mother is breastfeeding: “HPV vaccines can and should be given to breastfeeding women.” They explain that, because it’s not a live virus, there is no risk to the baby. They might want to educate themselves about the 500 mcg of aluminum, the polysorbate 80, and the sodium borate in the vaccine and whether or not these toxic substances can be passed to the baby before announcing that it is unequivocally safe. I could not find such evidence to “reassure” me.
Here is where we see the wheels come off. What happened to “first, do no harm” or the precautionary principle? ACOG has decided on a policy of not recommending a simple urine pregnancy test before vaccinating, even though the vaccine is contra-indicated for pregnant women. In the trials, of the girls who became pregnant within 30 days of receiving the vaccine, five babies were born with congenital birth defects as opposed to zero in the control group. This was explained away as coincidence because all the birth defects were different. Personally, I don’t find that reassuring either. However, it was raised as a safety flag by VRBPAC before the vaccine was approved, and the discussion can be found here.
There seems to be a push by scientists to support the idea that giving the vaccine during pregnancy is “not unsafe” as we are seeing more and more headlines like this one from Reuters: “HPV vaccination during pregnancy shows no ill effects.” Why would there be a need to study this if not to ward off potential lawsuits once the truth gets out? Why would there be a need to prove this vaccine is safe for pregnant women if there wasn’t some nefarious plan to add it to the now normal “pregnancy schedule”? But don’t, whatever you do, eat soft cheese or tuna fish.
The study this is based on was lacking for many reasons, but it does seem to be going out of its way to arrive at the (forgone?) conclusion that the vaccine is safe for pregnant women. What makes this study entirely irrelevant today, however, is that the data only looks at the quadrivalent vaccine which is no longer being given. Would double the dose of antigens and aluminum contained in Gardasil 9 make a difference to the outcome? We don’t know.
The study calls the control cohort “unvaccinated”; however, we don’t know if it means “not vaccinated with HPV but perhaps with flu or Dtap”? Since the trials indicated that the first 30 days were the most dangerous with regard to a baby’s health outcome, this study did not count spontaneous abortions, commonly known as “miscarriages,” within the first six weeks of pregnancy. I don’t see how it creates a scientific bias if those results are included. (Editor’s note: In fact, if the strongest adverse event is spontaneous abortion, this is a really good way to hide that fact.) And again, those real-world risk factors are being used to explain away data and cohorts are adjusted, according to the Reuters article;
Although the raw data did suggest higher rates of low birth weight, preterm birth and major birth defects, vaccinated women were also more likely to be smokers, unmarried and have both lower incomes and lower levels of education, putting them at higher risk for those outcomes in the first place. Once the research team adjusted for those factors, they found no significant difference in risk for women who got the vaccine while pregnant.
So there you have it. In the real world it’s rather dangerous, but in our controlled epidemiological study, we can make those danger signals go away once we see those signals pop up. Is this the new way of conducting scientific studies, manipulate the data? Where have we seen this before (Editor’s note: since we posted this blog, Dr. Thompson’s letter, via his attorneys, has been removed from the internet and so the link will take you to the wayback machine copy)? There is also no requirement for Merck to publish a negative-effect study, and so the published studies will always favor the sponsor in their outcomes. That’s just good business, and I guess the public just wants to be reassured, right?
I have no doubt that most, if not all, OB/GYNs are well intentioned and look to their parent organization for guidance in good faith. My issue with the position ACOG presents in its committee opinion is the push to vaccinate at all costs, at every chance, ignoring the risks, no matter what the long-term health outcomes are. Contributors to this controversy are ignoring the large swathe of reported vaccine injury cases all over the world, and instead taking comfort in being told that “the safety data for all three vaccines is reassuring.”
As for Merck pulling the strings over the ACOG, I don’t think anyone in the organization sees anything wrong with it. We are approaching this topic from two distinct positions and so will never agree. One side is dealing with devastating cancers and surgeries every day, and the other is hearing devastating cases of vaccine injury. The two are both very tragic but the latter more so because they are being ridiculed and maligned by the very doctors who should be there to help them. Doctors used to listen to patients but sadly not any more, at least where vaccines (and cancer) are concerned.
To dismiss these testimonies in favor of the “greater good” policy of making the HPV virus the biggest evil plague to befall our children, only to have the elixir right in every doctor’s office in the land, is egregious. To push this vaccine without a single reference to good sexual health practices, the vaccine’s duration, and mention of other risk factors for the disease is reprehensible. Doctors appear to be abandoning their commitment to their patients in favor of a devotion to this non-existent public health emergency and the potential of saving future lives. None of that can be shown to be true or ever proven, but the theory is profound. If the “safety is reassuring,” then it’s worth the risk, right? But the patient bears 100% of that risk, not the doctor, and especially not ACOG.
ACOG, and all the other organizations in partnership with Merck, are part of an orchestrated marketing strategy whether they know it or not, one that nets Merck over $2 billion in sales each year. The push to increase vaccination rates (via mandates) and ensure boys get the message too is going to come at a great cost to our children’s health whilst filling up Merck’s coffers. I’m sure that there is a bottomless legal fee contingency account to fill on their balance sheet, is my guess.
We cannot know the future, but we are already seeing a virtual killing field of casualties all over the world. Scientists and doctors may not see this right now because it’s all about the headlines and bottom-lines, but it’s coming. I hope I’m wrong, I do. But history tells me that I’m not. It has happened before with Thalidomide, Vioxx, DTP and other vaccines, and it’s happening now with Gardasil. Parents are up against an incredible amount of pressure from doctors, who can bully and coerce just by donning that white coat. Parents must ignore what’s in their heart and soul and offer up their children in blind faith. What they don’t know is that this faith is being placed in doctors who are themselves blinded, or who choose to be blinded, for the greater good. Orwell predicted it perfectly.
I hope and pray that one day they will see. In the meantime, we need to continue to sound the alarm and be the voice for those injured, who no longer have the energy to scream it from the rooftops.
“Be one less . . .”
~ ShamROCK
For more by ShamROCK, click here.







Thank you for such a well researched article. My only suggestion is to remove the meme that says “Helping destroy the lives of little girls one injection at a time” because it is what shows up when you share your article, and it implies that every little girl that gets the HPV vaccine is going to have her life destroyed. That is a statement that cannot be supported, whereas everything in your article can, and I’m afraid that people who want fact based articles (which this absolutely is) might be turned off by it. What about using the meme of a girl injured by the HPV vaccine that says something like “Don’t be one more” (a play on Merck’s marketing ad), if you want a graphic in that spot?
Thank you again for such a great article.
You bring up a good point. We aren’t really meme makers though, and nobody shares an article unless it has a picture attached. If you know anyone who could make us one with something like “Be One Less… Girl (or Boy) Injured by Gardasil.” We’d be happy to change it.
Thank you for the amazingly well researched article. What a horror show this vaccine has turned out to be. HPV itself is a terrible illness, but we seem to be using an equally dangerous and terrible prevention tactic, when we probably need something more like a social services based approach targeting high-risk populations. My baby daughter was vaccinated for HPV at 6 months, the doc didn’t even tell me it was optional and a clinical trial. I found out later when he tried to do it again and I asked why he was vaccinating her a second time under the age of 3 for HPV and he said it was because the first one wasn’t effective for long enough. That was all before my eyes were opened by my son’s massive regression into autism/PANS.
I called into the Advisory Commission on Childhood Vaccines a year or so ago while they were raking the manufacturer over the coals because of this vaccine and the, in their opinion, inadequate safety studies, but that was when there had only been 100 deaths. I guess they knew more were coming. Too bad it’s a toothless organization that could do nothing but kick back and watch.
I hope to God my daughter’s reproductive system wasn’t harmed by that needless vaccine. Some teens are reporting that it triggered menopause.
Ruth,
Are you saying that your 6 month old baby was vaccinated for HPV without your consent as part of a trial? That’s medical battery and you should talk to a lawyer. If he was conducting a trial on babies, it should be reported, you should have been informed. This is outrageous.
Also HPV is not a terrible disease, it’s not even a disease, it’s an infection (which clears most of the time). Cervical cancer is a terrible disease which can be prevented and treated.
I’m sure your daughter will be fine, please don’t worry. But I would talk to someone about reporting that doctor for malpractice.
Best of luck
https://jonrappoport.wordpress.com/2017/04/24/julie-and-the-boys-cdc-merck-vaccines/
But what about Stephen Kraling and Joan Wlochowski?
Who?
They’re two former Merck virologists who filed a qui tam suit against Merck, the manufacturer of the very same MMR vaccine. (Ref: Federal Civil Lawsuit: UNITED STATES OF AMERICA et al. v. MERCK & CO., Pennsylvania Eastern District Court, Case No. 2:10-cv-04374-CDJ, District Judge C. DARNELL JONES, II, presiding)
The suit claims Merck defrauded the US government by selling the vaccine, under a federal contract, when Merck knew the mumps component of the vaccine was far less effective than advertised.
Of course, Merck disputed this claim, but on September 5th, 2014, Judge Jones, of the Federal District Court for the Eastern District of Pennsylvania, gave the green light for the suit to move forward.
Kraling and Wlochowski assert several levels of Merck fraud:
To achieve a slam-dunk success, Merck tested the effectiveness of the MMR vaccine against the version of the virus in the vaccine, rather than against the natural mumps virus a person would catch in the real world.
Merck irrelevantly and deceptively added animal antibodies to the test results, thus giving the false appearance of strong human immune response to the vaccine.
On top of that, Merck faked the quantitative results of the tests to which the animal antibodies had been added.
Great article. Thanks.
Thank you Rebecca! Please share!